


 QCS is here to help you gather all the evidence you need for the new CQC inspections
QCS is here to help you gather all the evidence you need for the new CQC inspections

This article will expand on the approaches to evidence gathering which the CQC will use.
Evidence gathering
The CQC says that their intelligence gathering system is called Intelligent Monitoring, and it is used to identify when where and what to inspect. This approach is key to their policy of targeting scarce inspection resource where it is most needed.
A previous article explained that the 11 Fundamental Standards are monitored by asking 5 Key Questions, each of which are themselves expanded into several Key Lines of Enquiry (KLOEs). Similarly to the previous Outcomes, each KLOE is further expanded into a set of Prompts, which are in effect the key performance indicators for the KLOE. Some, but not all of the KLOEs are listed as “Mandatory”, which means that they will be assessed at every inspection. The other KLOEs are to be inspected on a different schedule, and it is this schedule which will be informed at least in part by the Intelligent Monitoring process. KLOEs which have been indicated through Intelligent Monitoring as a potential risk area will be added to the next inspection schedule for that Service, or trigger an out of schedule on-site inspection.
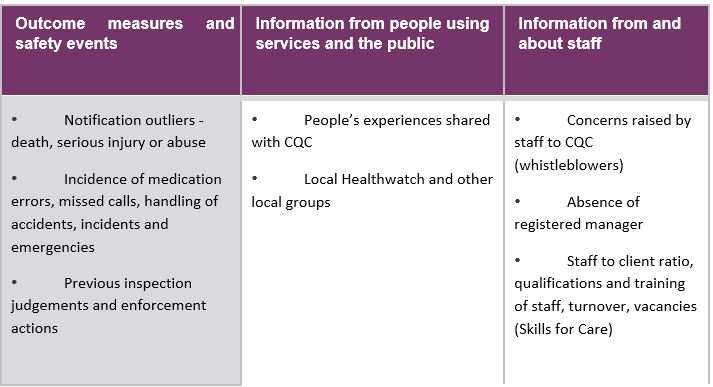
Some of the sources of intelligence are explained in the CQC publication Provider Handbook – Consultation, section 4, page 20.
Healthwatch
CQC explain, in Provider Handbook – Consultation, section 3, page 15 that:
Local Healthwatch staff and volunteers work to make sure the voices and experiences of people who use services, carers, families and the public are heard. They also influence the planning, provision and improvement of health and social care services and represent people’s views on the health and wellbeing boards set up by local authorities. We will have a regular and two way relationship with local Healthwatch in every area, giving them the opportunity to share their evidence about social care services including their ‘enter and view’ reports when they have visited services themselves. We will coordinate our inspection plans with their enter and view programme to ensure we are not both visiting services at the same time.
- Statutory notifications
- Safeguarding alerts
- Reports from users of services
- Reports from staff
- Reports from the public
Notifications of all these data will be viewed by the CQC individually, and also examined for negative trends. The QCS system encourages and facilitates a simple administrative system to record all notifications to simplify regular trend review for Quality Assurance purposes.
To illustrate the approach, the CQC have published a draft example of sources of intelligence in their publication Provider Handbook – Consultation, section 4, page 21.
This process has been in use by the CQC for some years, ever since they moved from regular inspections to targeted inspections. However, Providers should not be complacent about the process simply because it has been around for some time. The CQC clearly state that while Intelligent Monitoring will inform risk assessment and may trigger further information gathering or an on-site visit, it will not be used on its own (our italics) to decide final judgements. The language indicates that Intelligent Monitoring may influence final judgements, together with other information, therefore all Providers need to be aware of and manage the flow of information arising out of their day to day operations. The days of the on-site inspection being the only factor in the final judgement have long gone, and lack of attention to information supervision could have negative consequences.
The QCS system is explicit about what information needs to be reported to the CQC, and how to do it. The intention is that through the exposure of all employees to the Policy and Procedure system, they are all aware of their reporting responsibilities to management, assisting the Registered Manager in maintaining the legally required level of notification.
Within the Quality Assurance model in the QCS system, data is managed in such a way that identifying trends, be they negative or positive, is enhanced and surrounded by action oriented mechanisms to make sure that responsive action takes place as a result.
The QCS care compliance system is being edited and updated to match the new standards, including the need for good information management and analysis. For instance, the matter of feedback to CQC from Service Users, families, professionals and employees should not be left to chance. The responsible Provider regularly surveys each of these groups. The objective is to identify dissatisfactions at an early stage and feed them into the service improvement management system before they reach crisis proportions, leading to reports to external agencies such as CQC. In other words, using surveys intelligently to drive the quality assurance process, rather than simply as a mechanism for a pat on the back. The design of the new QCS surveys has moved away from the traditional question-based format to a format which enhances the flow of information about their rights given to the Service User. This in turn meets one or more of the new KLOEs, a compliance not achieved by conventional survey methods.
QCS is providing a full suite of surveys to each group mentioned above, each survey focussed on one of the Key Questions. In addition, a totally revise Mock Inspection Toolkit is in preparation which will be split into two useful elements – first of all a statement of the processes, usually based on QCS Policies and Procedures, which need to be in place to produce the results expected by the Standards. This section will form a major part of the Provider’s compliance implementation plan. Secondly, we are providing a checklist of evidence which should be provided by the processes, enabling the Service to periodically audit that it is actually carrying out the required processes identified in part 1, and producing the required evidence. Planning and regular use of the Toolkit will give Providers the information they need to steer their Service along the path to full compliance with the Fundamental Standards.
Finally, on the subject of information, the CQC have introduced the Provider Information Return (PIR). This document is a modification of the familiar Provider Compliance Assessment, edited and expanded to match the Fundamental Standards. The CQC state that they have not yet decided if this will be regularly issued, or whether it will be a pre-cursor to inspection. It will primarily be available online.
Much of the updates which QCS is introducing into its compliance management system to meet the Fundamental Standards is aimed at assisting the Provider to gather the information required by the PIR over time, with the effect that the information should be more accurate, not compiled as a result of a last minute rush, and, critically, open for analysis throughout the data gathering period so that trends can be identified and managed. These may be negative trends which require correction, or positive trends which require building on.
Background
In Part 1 of the series we have seen how the Care Quality Commission has proposed to implement from October 2014 a new regime of registration and inspection in response to failures of the current regime to spot and deal with poor quality care before too many people were harmed.
We saw that the CQC proposes a new, clarified and re-focussed registration and inspection regime, demonstrated by the following schematic.
The schematic demonstrates that the CQC regard their overall registration process as having five steps, these being:
- Registration
- Intelligent Monitoring
- Expert inspections
- Judgement and publication
- Action, if indicated by the inspection outcome
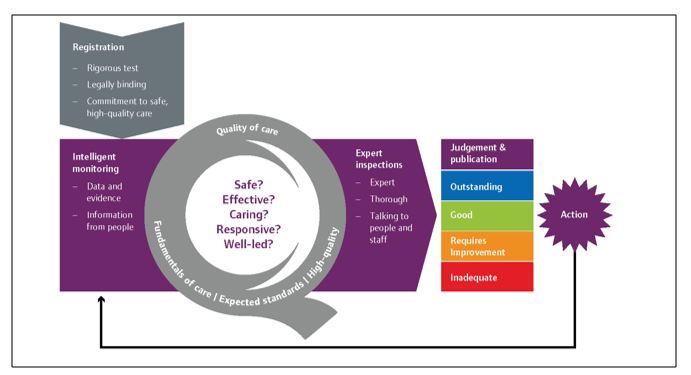
(Provider Handbook (Adult Social Care) Consultation, Page 2)
The scope of each of these processes is based on the new definitions of quality, these being:
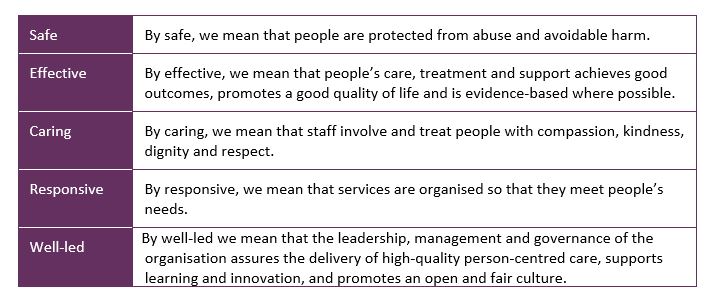
(Provider Handbook (Adult Social Care) Consultation, Page 2)
Michael Dempsey – QCS Compliance Director