

 Last week we began to take a look at creative art, or higher arts, such as – classical music, painting, literature etc. When the areas of the brain designed to allow us to comprehend and make sense of these arts, and to impart ‘meaning’, are so catastrophically damaged by the ravishes of most dementia, particularly dementia of the Alzheimer’s type, can a person could still garner pleasure, comfort or ‘restoration’ from the use of these subjects and objects as therapy?
Last week we began to take a look at creative art, or higher arts, such as – classical music, painting, literature etc. When the areas of the brain designed to allow us to comprehend and make sense of these arts, and to impart ‘meaning’, are so catastrophically damaged by the ravishes of most dementia, particularly dementia of the Alzheimer’s type, can a person could still garner pleasure, comfort or ‘restoration’ from the use of these subjects and objects as therapy?
This week we look at a theory which suggests that at certain ‘stages’ within the more destructive dementias the person would indeed receive none to little benefit from the use of such therapeutic use of ‘art.’ In the coming weeks we will look at other models which suggest radically different interpretations of the inner world of someone living with a dementia, and as to why art may be one of the most powerful mediums for ‘reaching’ and releasing inner emotions.
‘I’m still here’
It is vital that older people feel worthwhile, that they have a sense of self-actualisation and control and that they feel they can contribute and hold influence over their own lives. You will have understood from our dialogue across the last few months that I strongly argue that when someone, for whatever reason, is unable to meet their basic and higher physical, social, psychological and spiritual needs, we as paid carers must develop the knowledge, skill and will to adapt the built and social environments to compensate for this inability.
If we look closely at those people living with us, and then assess through their eyes, which areas of their daily contribution to the life of the care home we could enhance to meet the above needs, without a doubt it is the level and degree of activities and occupation.
Activities need to be designed to meet the basic need for inclusion and involvement, and each person individually needs to be meaningfully occupied. Activities should not be childlike, should be able to be undertaken in groups and individually, should be created around a strengths-based model, and the person should be able to choose to opt in or out. Everyone in your care should have a meaningful and ongoing assessment of their abilities to participate within an activity and occupation programme, and then this should be tailored to the person’s specific needs.
Where abilities are restricted, an activity should not force the person to confront their failings but should be designed to allow quick wins and victories. The Montessori methodology is very useful in this respect and should be a part of every carer’s repertoire. There are books and video’s available if you wish to study and apply the techniques – I urge you to seek these out and apply.
Bingo – really?
I don’t particularly like to watch paid carers playing Bingo – just something I am funny about. But in most care homes I visit – and it’s a lot – I see Bingo on the daily activities board – and I become immensely suspicious
So I go along to the residents’ Bingo activity and I see a couple of carers, sometimes nurses, often, if not always the ‘activity co-ordinator’, and they are playing three, maybe four cards themselves, They are usually surrounded by residents looking on helplessly and occasionally laughing at the appropriate social cues, whenever a housey house is called, and I think ‘who is this activity for?’
When I enquire if the people ‘playing’ can actually read the numbers on the card, follow the sequencing of the numeral patterns, understand the concept of the caller, the number, the relationship of the call to the numbers on the card, the searching for the number, the locating of the pen, the marking of the correct number, the realisation that a full house is achieved and its significance, and then the knowing of when to shout ‘Bingo’, I am looked at blankly, or worse, with suspicion or unadulterated hatred! (Don’t worry I always think, you will get used to it. I never do)
Invariably of course the answer is ‘we play for them’
Now, for every person who can do all the above and loves the social milieu, great, but for all who cannot, but who still need the social involvement and interaction, please remember my thoughts on care streaming. Find an activity or occupation, through ongoing assessment, that really works for the person, and allows them to participate, to win, to feel in control and not compromised by playing a game that was once second nature, but now only seeks to show how far they have fallen…
One of the well-known figures currently working in dementia care is the occupational therapist Tessa Perrin. She and others who follow her occupational models work in applying stage thinking to occupation and activity in dementia. This thinking offers a models we can apply that will make activity work productively at all ability levels.
Simply put, her ‘developmental model’ offers Piaget’s developmental theories in reverse. Piaget was, among other things, a psychologist who was interested in cognitive development. After the observation of many children, he posited that children with normal development (that is, without any cognitive disability) progress through four stages and that they all do so in the same order.
These four stages
- The sensorimotor period (birth to 2 years). During this time, Piaget said that a child’s cognitive system is limited to motor reflexes but the child builds on these reflexes to develop more sophisticated procedures. They learn to generalise their activities to a wider range of situations and coordinate them into increasingly lengthy chains of behaviour.
- Preoperational thought (2 to 6/7 years). At this age, according to Piaget, children acquire representational skills in the areas of mental imagery, and especially around language. They are very self-oriented, and have an egocentric view; that is, preoperational children can use these representational skills only to view the world from their own internal perspective.
- Concrete operations (6/7 to 11/12). As opposed to preoperational children, children in the concrete operations stage are able to take another’s point of view and take into account more than one perspective simultaneously. They can also represent transformations as well as static situations. Although they can understand concrete problems, Piaget would argue that they cannot yet perform on abstract problems, and that they do not consider all of the logically possible outcomes.
- Formal operations (11/12 to adult). Children who attain the formal operation stage are capable of thinking logically and abstractly. They can also reason theoretically. Piaget considered this the ultimate stage of development, and stated that although the children would still have to revise their knowledge base, their way of thinking was as powerful as it would get.
Adaptation: assimilation and accommodation
In Piaget’s theory of development, there are two cognitive processes that are crucial for progressing from stage to stage: assimilation and accommodation.
- Assimilation. This refers to the way in which a child transforms new information so that it makes sense within their existing knowledge base. That is, a child tries to understand new knowledge in terms of their existing knowledge. For example, a baby who is given a new object may grasp or suck on that object in the same way that they grasped or sucked other objects.
- Accommodation. This happens when a child changes their cognitive structure in an attempt to understand new information. For example, the child learns to grasp a new object in a different way, or learns that the new object should not be sucked. In that way, the child has adapted their way of thinking to a new experience.
Taken together, assimilation and accommodation make up adaptation, which refers to the child’s ability to adapt to their built and social environment.
It is worth noting that it is thought now that not every child reaches the formal operation stage and that developmental psychologists now debate whether children do go through the stages in the way that Piaget postulated at all.
Whether Piaget was correct or not, it is safe to say that this theory of cognitive development has had a tremendous influence on all modern developmental psychologists and it is relevant to our understanding of the complexities of dementia caring and specifically may help with using assessment to plan activity and occupation within a care centre or care homes.
Perrin’s model demonstrates three types of ability level that spans four stages of dementia: early, early to mid, mid to late and late.
(The validity of this model may be contested, especially as there are many types of dementia. Perhaps thinking does not disassemble in the same way as it assembled, however, as a way of simply explaining the need to apply varying activity and occupation programmes for those living with a dementia, it is hard to beat the applicability of the approach.)
One of the problems, of course, when using a stage theory is that most people, most of the time, will either be in two or more categories simultaneously and thereafter constantly fluctuate between grading determinants. But as you can see from the diagram below a delineation of this sort can prove helpful when designing for ability.
Utilising ‘care streaming’, in which people are cared for in smaller groups based around shared abilities and weaknesses, allows us to be more accurate and much less concrete in our caring. (The Pool Assessment Tool is an excellent resource in achieving this methodology.)
TABLE 1.1 Perrin’s formulation

TABLE 1.2 Nature of stage and abilities suggested for the three main groups
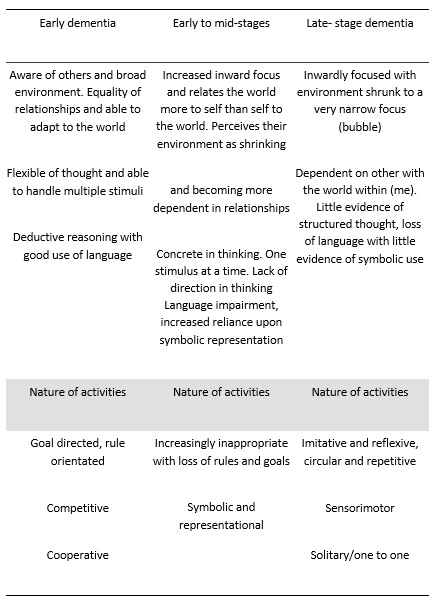
If we use these broad areas to look at the type of abilities suggested for each of the three main groups we find the following associations with matching ability and capacity to activities that create win-win situations and allows the person mastery over the task at hand.
These concepts are generalisations but begin to provide ideas of the types of adaptations you can build into programs of activities and occupational based around the person’s individual profile and their assessed and constantly reassessed abilities
TABLE 1.3 Matching activity to ability level
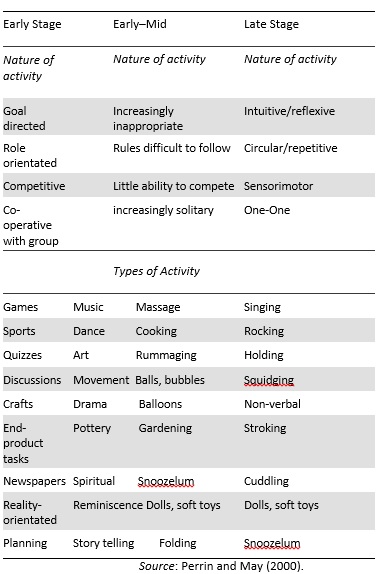
One of the most important aspects of designing activities or creating meaningful occupation is ensuring that the person is not outpaced; that is, avoiding any intervention that is too fast, too complex or too difficult for the person to cope with at any point in time.
Outpacing can result in the person being left lost, floundering and feeling helpless and belittled. This is not what you should be aiming for.
What we are aiming for is a match. With the correct use of assessment and the right choice of activity or occupation we have a win–win scenario. I consider that the model put forward by Perrin will go a long way towards creating rewarding win–win situations and I offer it as one of many for you.
Next week we will look at other models in our quest to understand if art remains relevant and valid to a person living with a dementia.
Till next time.
Paul Smith – Dementia Care Expert



