


 Last week we began to look at some of the biological causes of dementia, in particular we singled out the primary dementias and concentrated on DAT. The week before we looked at memory, memory systems and the processes by which memories are made – and lost.
Last week we began to look at some of the biological causes of dementia, in particular we singled out the primary dementias and concentrated on DAT. The week before we looked at memory, memory systems and the processes by which memories are made – and lost.
This week we look at the second most common form of the primary dementias, that of vascular dementia (VD), and we discuss some of the causes and some common symptoms. However to quickly recap: Every person living with a dementia is unique. Dementia itself is not an illness or any one specific disease process, rather it is a syndrome, a term used to describe a collection of related diseases and pathologies.
A syndrome is a collection of signs and symptoms that can be commonly grouped together and are recognised as producing a similar outcome even if the causes may be different.
There are well over 140 different types of ‘dementia’ and it is probable more will come to light in the next decade, however we said that the general public commonly believe that when any reference to ‘dementia’ is made we are referring to someone living with Alzheimer’s disease, but as you will read this week, often, we are not.
Vascular dementia – Whenever damage occurs to the structure of the brain or oxygen is reduced to the brain, cells die.
The symptoms of vascular dementia can occur suddenly or gradually following a stroke or several small strokes as these are events that A) damage the structure of the brain and b) reduce oxygen to the affected brain region.
If these events are large enough, or frequent enough, then damage will eventually reach a critical mass where global performance (the whole function of the brain) is affected. However VD differs markedly from DAT unless damage to the brain reaches critical levels and multiple brain regions are affected. In the early stages small TIA’s can leave a person with symptoms that can be mistaken for depression and if damage is concentrated to specific regions of the brain then only he functions these areas control may be affected.
Vascular dementia accounts for about 10 – 20 per cent of all diagnosed dementias and is usually seen in the seventh and eight decades of life. Pure vascular dementia is now thought less common than in previous decades, as the presentation of mixed dementia – a combination of cerebral incidents with the plaques and tangles of Alzheimers disease is now rising.
This is likely due to more sophisticated imaging technology and a greater awareness among GPs of the differences and similarities of the two, and may also be in part an outcome of the medical history that can be followed with the types of diseases that can lead to VD, as opposed to the diagnosis by omission most often applied to the symptoms of DAT.
The most common form of vascular dementia (VD) is multi-infarct dementia (MID) which follows a series of strokes, or infarcts.
The stroke may be ‘silent’ and pass almost unnoticed and these small almost imperceptible episodes are often referred to as ‘strokelets’, however, even in these instances, when enough brain tissue becomes destroyed the result will be dementia.
A stroke is what happens when the blood supply to part of the brain is cut off. Blood carries essential nutrients and oxygen to the brain. Without a blood supply, brain cells can be damaged or destroyed and won’t be able to do their job.
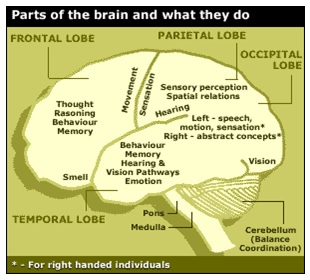
Because the brain controls everything the body does, damage to the brain will affect body functions. For example, if a stroke damages the part of the brain that controls how limbs move, limb movement will be affected. The brain also controls how we think, learn, feel and communicate.
A stroke is sudden and the effects on the body are immediate.
Infarction
Stroke can cause brain tissue to die, and this is called cerebral infarction. An infarct is an area of dead tissue. It can be tiny or affect a larger part of the brain.
Blood flow to the brain can be cut off by:
- A blockage (ischemic stroke)
- A bleed (hemorrhagic stroke)
The most common type of stroke is a blockage. This is called an ischemic stroke, which happens when a clot blocks an artery that carries blood to the brain. It may be caused by:
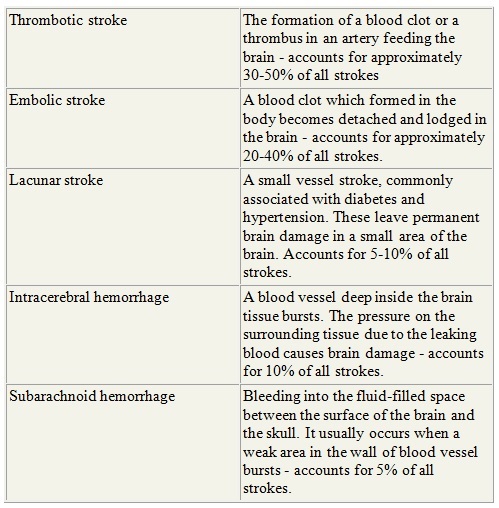
- A cerebral thrombosis, when a blood clot (thrombus) forms in a main artery to the brain
- A cerebral embolism, when a blockage caused by a blood clot, air bubble or fat globule (embolism) forms in a blood vessel somewhere else in the body and is carried in the bloodstream to the brain
- A blockage in the tiny blood vessels deep within the brain (lacunar stroke).
The second type of stroke is a bleed, when a blood vessel bursts, causing bleeding (hemorrhage) into the brain.
This is called a hemorrhagic stroke. It may be caused by:
- An intracerebral hemorrhage, when a blood vessel bursts within the brain
- A subarachnoid hemorrhage, when a blood vessel on the surface of the brain bleeds into the area between the brain and the skull (subarachnoid space)
Definitions of ‘Stroke’
Multi Infarct dementia (MID) is a remitting dementia characterised by an abrupt onset and progressing in steps rather than a continuous decline as in Alzheimer’s disease – this step like progression of course follows subsequent small strokes which may vary in their frequency, degree and location.
It is very important to seek medical input if suspected strokelets are occurring as often treatment to prevent further damage can be offered. Dead tissue however cannot be reanimated.
The damage can be local to the area of the brain affected until the degeneration becomes more widespread. After an initial episode there is usually some small recovery until the next time.
As some parts of the brain may be spared the picture we see in VD is inconsistent levels of performance and some unique behaviour as the person struggles to make sense of a brain that works well in some aspects and not at all in others.
Eventually, if damage continues and becomes more global the person begins to take on the general characteristics of someone living with DAT as multiple areas of function and cognition will be affected.
The ‘good news’ however is the discovery and therapeutic use of the fact that our brains are plastic – that is they can often adapt and accommodate injury and insult by having other areas pick up some or all of the abilities formally performed by a damaged area. Often this compensation process needs professional directing, the process can be sudden or prolonged but there is always hope with dementia. With treatment and rehabilitation vascular dementia has a sunnier prognosis than dementia of the Alzheimers type, which will generally continue to progress irrespective of attempts at treatment.
The early warning signs of vascular dementia can be very similar to those of depression and it is important that these signs are brought to the attention of a GP, as the condition cannot be stopped once the brain impairment progresses.
Early symptoms of vascular cognitive impairment
People with vascular cognitive impairment can experience a wide range of symptoms, such as slowness of thought, difficulty with planning, memory loss, trouble with language, and mood or behavioural changes.
At this early stage, the loss of mental ability may be barely noticeable, or mistaken for something else such as depression.
Difficulty with performance across these areas indicates that some brain damage has already occurred and treatment needs to be started immediately.
Symptoms of vascular dementia
Once the brain damage has progressed to vascular dementia, symptoms can worsen quite quickly as brain tissue begins to die.
Symptoms of vascular dementia depend on which area of the brain has been damaged.
The rate of progression varies during the course of the disease and from person to person. For example, the condition might be stable for several months or years, but strokes can then occur that lead to a sudden worsening of symptoms. Stress and psychological trauma as well as continued physical disease processes have been shown to precipitate sudden worsening of the condition.
Possible symptoms can include:
- severe slowness of thought
- feeling disorientated and confused
- memory loss and difficulty concentrating
- difficulty finding the right words
- severe personality changes, such as becoming aggressive
- depression, mood swings and apathy (unresponsiveness)
- finding it difficult to walk and keep balance, frequently falling
- having a frequent urge to urinate, without actually having a urological condition
- hallucinations (seeing or hearing things that aren’t there) and delusions (believing things that are not true)
It is possible to have a combination of vascular dementia and Alzheimer’s disease, and mixed dementia’s now account for the fourth largest percentage of diagnosis of dementia.
Till next time
Paul Smith – Dementia Care Expert



