


 Dementia acts as a stressor to the internal system of an affected individual by its alteration in perceptions of the external environment and therefore the individual’s reactions to it.
Dementia acts as a stressor to the internal system of an affected individual by its alteration in perceptions of the external environment and therefore the individual’s reactions to it.
External stimuli from the environment create the opportunity for appraisal. This refers to the person’s inner resources and their ability to cope with the presented challenges.
Dementia robs the person of their means of coping successfully with everyday challenges and experiences by reducing their capacity to appraise and predict. This creates stress.
This stress is chronic and is interspersed with acute episodes. Prolonged and compounded stress leads to the state of exhaustion.
This state results in permanent tissue damage, altered ability to cope further, flattened immune system response and to death by either opportunistic infections or by the result of damage done to essential life systems, such as heart, lungs, brain etc. This we have learned across the last series of blogs.
Bringing our learnings together
A caring regime where person-centred ‘new culture’ approaches are being used can be seen as aiding in effective coping with the external and internal demands of stressors.
The life history and biographical nature of person-centred approaches can help professionals in the formulation of a plan of care based not only on present ability levels, but also in assessing the strength of previous coping strategies and abilities and in using these to further strengthen present abilities.
My proposed caring model, however, goes beyond this present and past orientation and asks you to use predictive caring – most dementias are progressive so we should always be using predictive profiling.
Imagine someone living with cancer and the team treating the disease basing their care advice purely on the current symptoms of the disease and the person’s life story up till now – is this cancer going anywhere soon? It is not. This is because the team looks at the future impacts, uses their knowledge of past outcomes for people living with the same type of cancer, adds personalised factors and then creates a future treatment regime to take away the negative impacts and where possible get rid of the damn thing!
Someone who has never coped well with life’s stress and pressure is likely to be more susceptible to the ravages of the dementing syndrome than someone who has shown resilience and durability whatever life has thrown at them – this you have learned.
All approaches to physical, psychological, social and environmental care are to be assessed in the context of the challenges these provide to the individual. The possible impacts of these challenges are to be measured against the individual’s previous, present and future coping abilities.
Where coping abilities are felt to be inadequate, the approach of the carer must include stress- reductionist strategies which, in turn, must ensure than when unavoidable stress is caused, this must be alleviated before any intervention can be said to be ‘complete’. Strategies for achieving this in future care must be created in the plan of care – this you have also learned.
It is ‘common sense’ that if a disease process is progressive it is our role to understand what is happening, how it is currently impacting and what is likely to happen and how that will impact and then – to plan to minimise the negatives using the person’s past, present and future strengths and abilities married in close partnership with your skills, enthusiasm and knowledge. This is the ‘model’ my blogs are following for you. I call this an adaptive response approach.
You must not be passive in working with someone living with a dementia. As a paid carer you must be constantly proactive. You must act, not just in a palliative way which assumes nothing can be done but to make someone warm, comfortable, safe and fed, but in a way that is dynamic and future outcome focused where you can make a positive difference. You are the difference. Make that difference every day – that is the joy of working in dementia care. Make that difference count
Internal rhythms and ‘performance’ variation
Circadian, ultradian and diurnal rhythms are one possible key to understanding fluctuations in the daily performance levels of people affected with dementia that are not generally understood and acknowledged as a care factor.
Each of these pulsatile body rhythms causes a cascade of hormones to be released into the system and, as we have already shown, the stress reaction occurring during the person’s attempts to cope with the effects of dementia has already begun a series of internal disruptions to these rhythms, disrupting and stressing natural defences, immunity and new tissue growth.
These internal changes caused by prolonged stress and by constant arousal may have severely reduced or even turned off vital hormonal production, most of which the internal rhythms are responsible for regulating.
Our internal rhythm
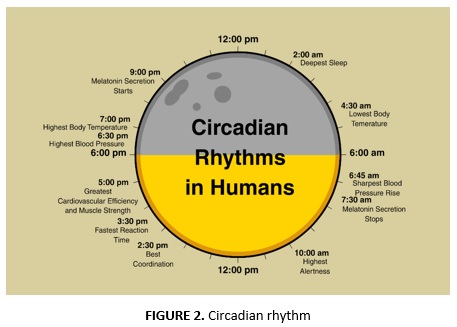
- Circadian rhythms. These occur about every 24–25 hours and have two major peaks, the late hours of the afternoon and the early hours of the morning. They affect and regulate body systems and impact everything from heartbeat to the clotting of blood. If certain areas of the brain are affected by dementia or other injury, circadian rhythms disappear completely and variations in function and regulation of hormones can begin to occur at totally random times of the day (Mestal, 1998). These are the same internal rhythms that are knocked out of cycle by ‘jet lag’ if you have experienced jet lag you can begin to appreciate what this feels like, both psychically and psychologically.
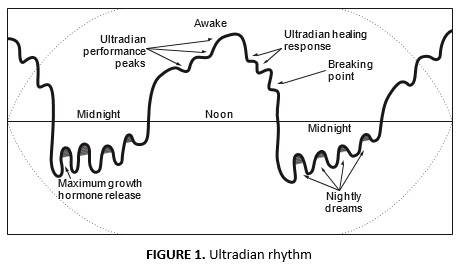
- Ultradian rhythms. These occur about every 90 minutes and are strongest at night and during sleep. Again these rhythms are responsible for cascading hormones and for enabling the various stages of sleep to be regulated.
- Diurnal rhythms. These occur throughout the day and account for people either being morning or night-time performers. As they play a part in consciousness and mental function, these rhythms can cause a severe worsening in both physical and especially psychological capabilities in either the morning or the afternoon (Dennett, 1991).
These internal rhythms, although disrupted by both age and stress, continue throughout our life span, but in periods of illness or stress may become varied in timing (Medina, 1996).
It is important to be aware of internal rhythms when considering the differing ability levels expressed by those people showing excessive swings in their performance of activities in daily living and in social interaction during the dementia experience.
It is also essential that we are aware that at certain times of both the day and night the person with dementia will be able to perform less well. Conversely, there may be times when the person is at a premium as regards to mental function and physical capability. These times can and should be built into any daily routines in order to maximise the person’s ability and experience of their ability. These rhythms will differ between individuals, but most people fall within the norms of circadian and ultradian function.
The effects on dementia of internal rhythms and their alterations precipitated by stress have yet to be fully explored. However, because this will entail internal temperature monitoring and will need full resident agreement and medical supervision, at present it is not a priority in dementia research or funding. This should not prevent us, however, from using already available research into healthy individuals’ reaction to these rhythms, and understanding that changes do occur and that performance is affected at times throughout both the day and night. If we plan for this, we will be encouraging the maximum potential of the person to be realised.
Stress, ‘sundowners’ and the breaking point
‘Sundowner’ or ‘sundowning’ are terms given to a collection of behaviours that occur with some people affected by dementia. They are most often more pronounced during the early evening period.
These behaviours include:
- restlessness
- increased agitation
- wandering, searching
- aggression
- shouting
- crying
- indiscriminate incontinence
- increased confusion
(Gross & McIlveen, 1999)
It should appear obvious that these are the same type of behaviours we encountered earlier in our exploration of stress and its effects. Could there be a possible link between the disruption to our bodily rhythms, the cumulative effects of stress on the person living with a dementia and the behaviours associated with sundowner?
When we couple these biological factors with the progressive damage to brain tissue and function that occurs throughout the dementia syndrome, it would seem obvious that these factors should link together. Also, it seems apparent that this link involves drops in function, with resultant cyclic changes in levels of behaviour and physical and psychological function and that this will impact social interaction, relationships and standing. It is also apparent that we can intervene to redress these negative impacts.
Reducing negative stress and compensating for cyclic functional variation
If this supposition is well-founded, it can be postulated that in line with the theory of degrees of dementia (the stage theory), and the effect on personhood and self-image of the social constructs of dementia (that it is others that often determine the quality of life and experience of someone living with a dementia), that the more positively the dementia experience is lived, the less affected by these changes the person would be.
In the physical reality of dementia care, it would appear that those who are engaged in a negative dementia experience are also those who tend to exhibit these dramatic ‘sundowner’ changes.
Based on this as yet unconfirmed position, I would suggest that a model such as adaptive response, which is based on regulation of stress, and ensuring the adequate provision of sleep and a strengthening of internal conditions by diet and carer proactivity, would allow for a re-regulating of bodily rhythms, or at least a realignment of performance. It would remove or reduce the experience of the negative effects of ‘sundowner’ (we will return to sundowning in a later blog).
Disturbed behaviours may be the result of altered body rhythm or the effects of unresolved stress upon the person. Helping the person to achieve undisturbed sleep and providing stress- free environments may help in the immediate alleviation of some ‘negative’ symptoms.
Next week I wish to bring you an insight into the work of Dr John Zeisel and to look at how his ideas with therapy using the arts is changing the way we think about care possibilities. I hope to show how the blogs we have been sharing link closely with why his approach works, and how the biopsychosocial ideas we have been exploring will help you adapt these approaches to your care settings.
Till next time.
Paul Smith – Dementia Care Expert



